
A breakthrough imaging technique is transforming the treatment of drug-resistant epilepsy by enabling doctors to pinpoint elusive brain lesions.
At Addenbrooke’s Hospital in Cambridge in the UK, ultra-powerful MRI scanners are now identifying subtle differences in brain tissue that were previously undetectable, prompting a reassessment of treatment plans for 58% of patients in a recent study.
One study participant, Amanda—a medication-resistant epilepsy sufferer whose lesion was located on the amygdala—experienced life-altering results following her surgery.
“Once I’d had the surgery, despite all the healing, it was very obviously the right decision,” she says. “Suddenly I realised I’m able to do loads of other things. It made me start to think, oh, what can I do? Things felt a lot more possible, like suddenly I’m able to do so many more things.”

Epilepsy, a chronic brain disorder affecting around 50 million people worldwide, causes recurrent seizures that can severely disrupt daily life. For approximately one-third of sufferers, medications fail to control these episodes, leaving surgical removal of lesions as the only viable option.
“Having epilepsy that doesn’t respond to anti-seizure medications can have a huge impact on patients’ lives, often affecting their independence and their ability to maintain a job,” says Dr Thomas Cope from the University’s Department of Clinical Neurosciences. “We know we can cure many of these patients, but that requires us to be able to pinpoint exactly where in the brain is the root of their seizures.”
A new technique in focus
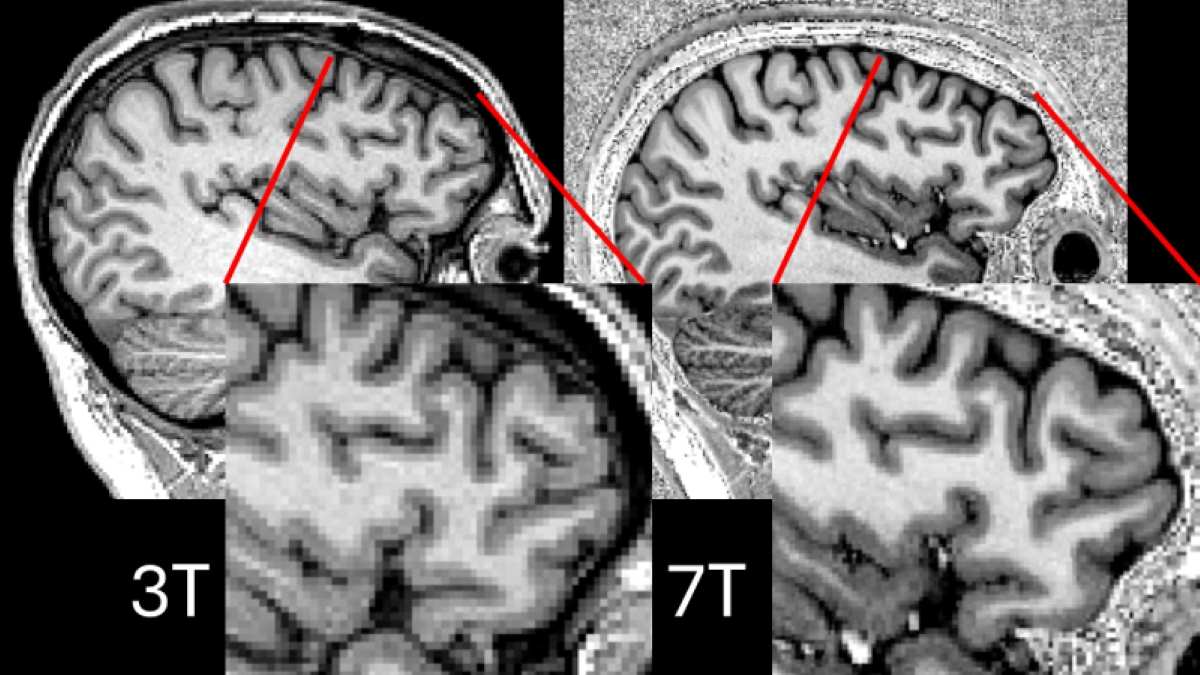
Magnetic resonance imaging (MRI) is a key tool in diagnosing epilepsy, with industry standards typically relying on 3T scanners. These machines, operating at 3 tesla (a measurement of magnetic field intensity), provide sufficient resolution for many clinical cases but can sometimes miss the very subtle brain lesions responsible for drug-resistant epilepsy.
In contrast, 7T scanners—using an even higher magnetic field strength—yield significantly finer image detail, which is crucial for identifying elusive epileptogenic lesions that may be targeted for surgical intervention.

However, conventional 7T scanners have struggled with signal dropouts—dark areas in the scans, particularly in the temporal lobes where most epilepsy cases originate.
To overcome this limitation, the team at the University of Cambridge’s Wolfson Brain Imaging Centre, in collaboration with colleagues at the Université Paris-Saclay, trialled a method called “parallel transmit.” Unlike traditional MRI scanners that use a single radio transmitter, parallel transmitters use eight transmitters arranged around the head. This configuration dramatically reduces dark spots and produces clearer, more precise images.
The research is published in Epilepsia.
“It used to be the case that MRI scanners used a single radio transmitter, but in a similar way to how single WIFI routers leave areas where you will struggle to get a signal, so these scanners would tend to leave blackspots on brain scans where it was hard to make out the relevant tissue,” explains Chris Rodgers, Professor of Biomedical Imaging at the University of Cambridge.
“Now, by using multiple radio transmitters positioned around the patient’s head – like having a WIFI mesh around your home – we can get much clearer images with fewer blackspots. This is important for epilepsy scans because we need to see very precisely which part of the brain is misbehaving”.
Testing on 31 patients with drug-resistant epilepsy, researchers found that the parallel transmit 7T scanner identified previously unseen structural lesions in nine patients. It confirmed in four patients suspected lesions detected using 3T scanners, and in a further four patients showed that suspected lesions could be disregarded.
Explainer: epilepsy
The improved clarity of parallel transmit 7T images led to significant changes in patient management. For 18 of the 31 patients (58%), the enhanced imaging results prompted a reassessment of their treatment plans. Notably, nine patients were offered surgery to remove the lesion, and one patient was offered laser interstitial thermal therapy (which uses heat to remove the lesion).
